Pragmatic Approaches to Assessing Physical Withdrawal in Clinical Trials
In drug research and development, understanding how a therapy behaves not only during treatment, but also after discontinuation, is essential to building a complete safety and efficacy profile. For central nervous system (CNS)-active therapies in particular, physical dependence and withdrawal can significantly influence both clinical outcomes and real-world use. As clinical trials evolve to become more patient-centric and efficient, sponsors are increasingly challenged to integrate robust withdrawal assessments without overburdening participants or compromising data quality.
In this blog, we explore the practical considerations for evaluating physical withdrawal in patient studies, offering a methodological framework to guide assessment strategies, which was originally presented in a scientific poster by Denise Milovan, Senior Scientific Advisor (Pharmacodynamics), Altasciences, et al. at the College on Problems of Drug Dependence (CPDD). Drawing on these insights, this article further examines how such approaches can balance scientific precision with operational feasibility, an increasingly important priority in today’s clinical research and drug development landscape.
Understanding the Role of Withdrawal in Clinical Research and Clinical Trials
Physical dependence is a physiological adaptation that occurs following repeated exposure to a drug, with withdrawal symptoms emerging after abrupt discontinuation or dose reduction. While often conflated with addiction, dependence is a distinct phenomenon that can occur even in the absence of abuse potential.
In clinical trials, particularly Phase II and III efficacy studies, the evaluation of withdrawal plays a critical role in shaping how a therapy is ultimately understood and used. Beyond simply identifying adverse effects, these assessments contribute to building a comprehensive safety profile, helping determine whether tapering strategies may be required at discontinuation, and informing regulatory decision-making, including the assessment of abuse potential and potential drug scheduling requirements.
The clinical significance of this work becomes clear when considering the range of possible withdrawal effects. Symptoms may be mild and transient for some therapies, but for others, they can be severe, complex, and in certain cases even life-threatening. Capturing this full spectrum is essential, not only for regulatory approval, but also for ensuring that treatments can be used safely and effectively in real-world settings.
Designing Withdrawal Assessments into Your Clinical Trials
In practice, evaluating physical withdrawal is rarely straightforward. While regulatory guidance outlines key expectations, translating these into large-scale, outpatient clinical trials introduces both scientific and operational complexity.
Withdrawal is most often assessed following abrupt discontinuation of the investigational product within Phase II and III efficacy studies, as part of a randomized withdrawal design, or through dedicated early-phase trials. Embedding these assessments into patient studies allows for observation of both withdrawal symptoms and potential rebound effects within the intended treatment population. However, this advantage comes with added demands on study design.
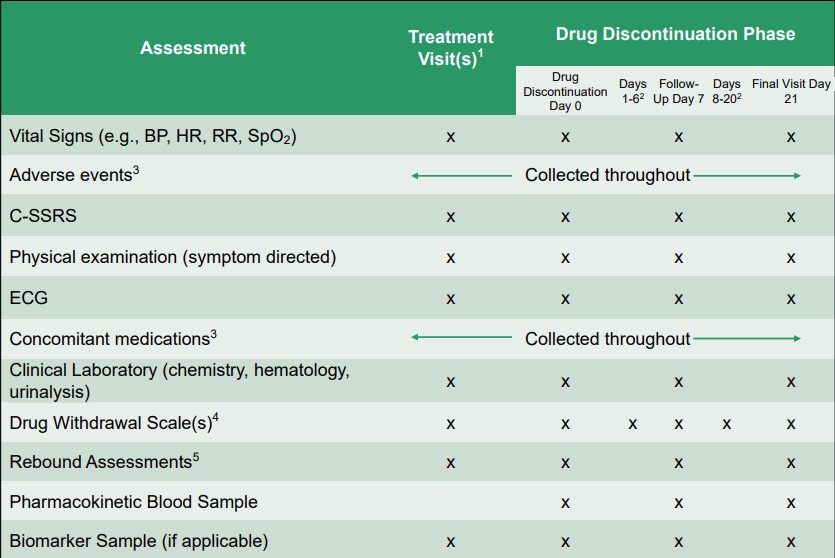
A meaningful assessment of physical dependence requires more than a single measurement approach. Instead, we recommend a coordinated framework that integrates multiple data streams, including clinical, patient-reported, and physiological, over a defined discontinuation period.
At a high level, this includes the use of:
- Withdrawal scales (drug-class or disease-specific)
- Adverse event monitoring before and after discontinuation
- Patient-reported diaries or electronic reporting tools
- Pharmacokinetic and pharmacodynamic correlations
- Physiological measures, such as vital signs or specialized metrics, that may require specific equipment or investigator training
Together, these components form the backbone of a comprehensive withdrawal assessment strategy, enabling a more complete understanding of how symptoms emerge, evolve, and resolve over time.
The table summarizes key methodological considerations for evaluating physical withdrawal symptoms in patient efficacy studies.
Navigating Real-World Challenges of Withdrawal Assessment in Clinical Trials
While the withdrawal assessment framework is conceptually solid, its implementation in real-world clinical trials presents several challenges, many of which stem from the realities of outpatient study design.
Feasibility
One of the most significant limitations is feasibility. Frequent in-clinic visits, often required for clinician-administered scales or physiological measurements, can place a considerable burden on participants. This is particularly relevant when withdrawal symptoms must be tracked daily or over extended follow-up periods.
A key theme in improving feasibility is the shift toward patient-centric, technology-enabled data collection. Digital tools, such as electronic diaries and mobile applications, can support more frequent, real-time symptom tracking without increasing the need for in-person site visits—helping reduce participant burden while improving data granularity and allowing study teams to monitor symptoms more closely between scheduled assessments.
Withdrawal Scale
At the same time, the tools themselves are not always ideally suited to the populations being studied. Many withdrawal scales were originally developed in populations with substance use disorders. For example, the Clinical Opiate Withdrawal Scale was developed for opioid withdrawal assessment and may be less directly applicable when evaluating withdrawal from non-opioid CNS-active therapies or investigational drugs with novel mechanisms of action. As such, its terminology and constructs may not translate well to broader patient groups.
To ensure relevance and clarity for broader patient populations, consider adapting the withdrawal assessment tools with the study group in mind. Modifying withdrawal scales can reduce potentially stigmatizing language, and thereby enhance both patient engagement and data reliability.
Solution: Safety Data Interpretation
Distinguishing between different clinical phenomena presents another challenge. Withdrawal symptoms must be carefully differentiated from the recurrence of the underlying disease, rebound effects related to discontinuation, and new or unrelated adverse events. This distinction is critical for accurate safety interpretation, but it can be difficult to achieve without sufficient data and context.
Planning for withdrawal assessment early in drug development, including the use of insights from nonclinical studies, can support more targeted assessment strategies in later-phase trials. Integrating pharmacokinetic and pharmacodynamic data with clinical observations is also essential for interpreting withdrawal effects within the broader clinical context of the therapy.
A Pragmatic Path Forward
While these approaches can help address several key methodological challenges, important operational and analytical limitations still remain. Compounding this, there is no standardized adverse event term specifically for drug withdrawal within commonly used clinical trial frameworks, requiring investigators to document both an overall withdrawal diagnosis and individual symptom-level adverse events separately.
From an analytical perspective, inconsistencies between spontaneously reported adverse events and structured questionnaire data can further complicate interpretation. In addition, limited sampling, whether due to study design constraints or patient burden, may obscure the timing and progression of withdrawal syndromes, particularly for drugs with longer half-lives or active metabolites.
While these approaches can improve feasibility and data richness, their effectiveness still depends on patient compliance and the reliability of self-reported data.
Understanding how drug exposure relates to symptom onset, duration, and severity enables more informed, clinically relevant conclusions, supporting more effective clinical trial design and higher-quality drug development programs.
How Altasciences Can Help With Your CNS-Active Drug Clinical Trials
Led by a team of experienced Principal Investigators, clinicians, and neuroscientists, we can design and execute even the most complex early-phase CNS trials, supporting sponsors from nonclinical assessment through clinical proof-of-concept, all within a single, streamlined framework. With over 30 years of experience and more than 200 CNS studies completed, our solutions span a broad range of neurological and psychiatric indications, including programs focused on cognition, pain, sleep, and behavioral health, across both healthy volunteer and patient populations.
Using validated models and cognitive assessments, you will receive high-quality data that drives informed decisions in early pharmacology, safety, and proof-of-concept outcomes.
Get in touch to learn how our experts can help you evaluate your CNS programs with precision and confidence.
This blog was originally published in June, 2026.
FAQ: Clinical Trials and Drug Withdrawal
Why is it important to assess withdrawal in clinical trials?
Assessing withdrawal in clinical trials helps define a drug’s safety profile, informs discontinuation and tapering strategies, and supports regulatory evaluations related to abuse potential and patient risk.
Are physical dependence and addiction the same?
No. Physical dependence refers to physiological adaptation and withdrawal symptoms after discontinuation of a medicinal product, while addiction involves compulsive drug use despite negative consequences.
What challenges are associated with measuring withdrawal in patient studies?
Common challenges include participant burden from frequent assessments, limitations of existing withdrawal scales, difficulty distinguishing withdrawal from disease recurrence, and variability in patient-reported data.



